NCLEX pediatric nursing content is tested across the health promotion and maintenance category and throughout physiological integrity, making it one of the most cross-cutting content areas on the exam. Many nursing students underestimate pediatric content because it represents a smaller percentage of the overall exam than cardiovascular or respiratory nursing — but the clinical reasoning demands of pediatric questions are just as high, and the specific knowledge required is distinct enough from adult nursing that unprepared candidates consistently miss these questions.
The most important foundational principle of NCLEX pediatric nursing is that children are not small adults. Their anatomy, physiology, developmental stage, response to illness, and psychosocial needs differ fundamentally from those of adult patients — and the NCLEX tests whether you understand and apply those differences in clinical scenarios. A respiratory rate that is normal for an adult indicates distress in a toddler. A medication dose that is appropriate for an adult is potentially lethal for a child. A nursing communication approach that is effective with an adult may be developmentally inappropriate for a school-age patient. These distinctions are at the heart of every NCLEX pediatric nursing question.
This guide covers the must-study NCLEX pediatric nursing topics for 2026 — growth and development, respiratory conditions, cardiovascular defects, neurological emergencies, child safety, immunizations, and family-centered care. Each topic is presented through the clinical reasoning lens the NCLEX applies, with priority nursing assessments, expected versus unexpected findings, and the patient and family teaching points that appear most consistently on the exam.
Growth, Development, and Family-Centered Care in NCLEX Pediatric Nursing
Growth and development is the conceptual foundation of NCLEX pediatric nursing. Every clinical decision in pediatric care — from how to communicate with a patient to how to involve the family in care planning — is shaped by the child’s developmental stage. The NCLEX tests this knowledge through questions that ask which nursing action is most developmentally appropriate, which response to a child’s behavior reflects accurate developmental understanding, and how to adapt patient teaching to the child’s age and cognitive level.
Developmental Milestones by Age Group
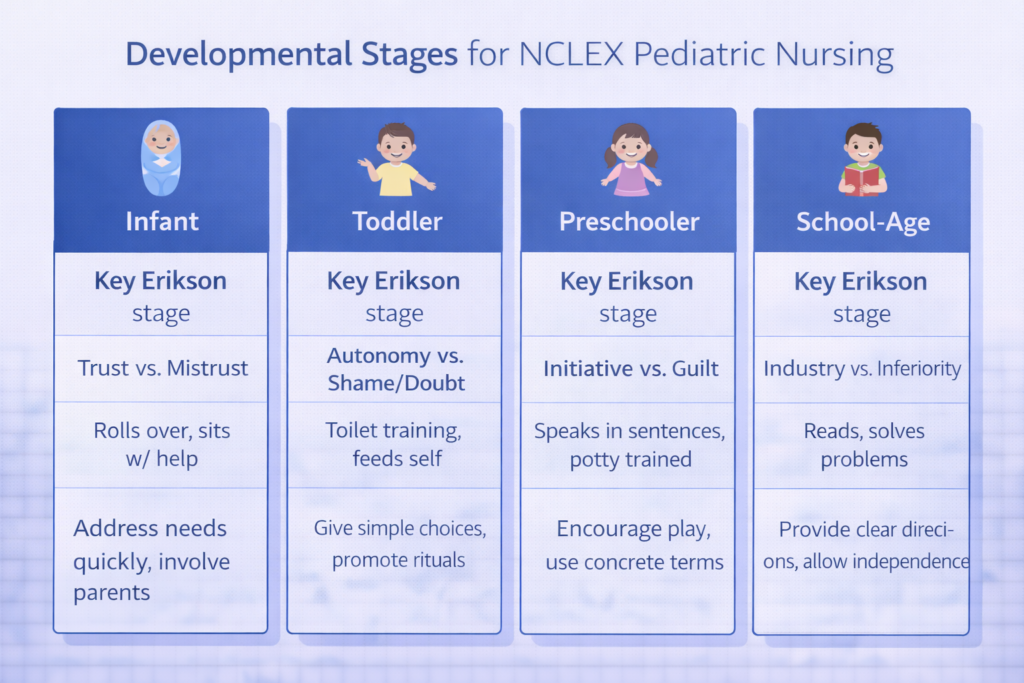
For NCLEX pediatric nursing purposes, know the major developmental milestones across four age groups. Infants (birth to 12 months) develop from reflexive behavior to purposeful movement, progressing through head control at 3 to 4 months, rolling at 5 to 6 months, sitting independently at 6 to 8 months, and walking with support by 9 to 12 months. Language develops from cooing to babbling to single words by 12 months. Toddlers (1 to 3 years) are characterized by Erikson’s autonomy versus shame and doubt stage — they assert independence, have frequent temper tantrums, and respond best to limited choices rather than open-ended decisions. Preschoolers (3 to 6 years) are in the initiative versus guilt stage, engage in magical thinking, fear body mutilation, and benefit from honest, concrete explanations about procedures. School-age children (6 to 12 years) are in the industry versus inferiority stage, can understand cause and effect, benefit from explanation of procedures in advance, and value peer relationships. Adolescents are in the identity versus role confusion stage and prioritize privacy, peer acceptance, and autonomy in healthcare decisions.
Erikson’s Psychosocial Stages in NCLEX Pediatric Nursing
Erikson’s psychosocial stages are high-yield NCLEX pediatric nursing content because they directly inform nursing interventions at every developmental stage. For infants, the priority nursing intervention that supports trust versus mistrust development is prompt, consistent response to the infant’s needs — pain management, feeding, and comforting on demand. For toddlers, offering limited choices — ‘do you want to hold your parent’s hand or the nurse’s hand during this procedure?’ — supports autonomy while maintaining safety. For preschoolers, allowing them to handle equipment before a procedure and using play therapy addresses magical thinking and fear of body mutilation. For school-age children, explaining procedures clearly and involving them in their care plan supports industry and self-efficacy. For adolescents, ensuring privacy, speaking directly to the patient rather than only to the parent, and addressing confidentiality explicitly supports identity development.
Family-Centered Care
Family-centered care is the organizing framework of NCLEX pediatric nursing. The family — particularly the primary caregiver — is recognized as the constant in the child’s life and as an essential partner in care planning and delivery. NCLEX pediatric nursing questions test your understanding of how to involve the family effectively: including parents in bedside care and teaching, assessing family coping and teaching needs alongside the child’s clinical needs, and recognizing when family anxiety or coping difficulty requires its own nursing intervention. For hospitalized children, rooming-in — allowing a parent to stay with the child continuously — is a standard of family-centered pediatric care that the NCLEX consistently supports as the correct nursing approach.
Respiratory Conditions in NCLEX Pediatric Nursing
Respiratory conditions are the highest-yield clinical content area within NCLEX pediatric nursing. Children are particularly vulnerable to respiratory compromise because their airways are smaller, their respiratory muscles are less developed, and their respiratory rates are higher at baseline — meaning that compensation for respiratory distress is limited and deterioration can occur rapidly.
Croup Versus Epiglottitis
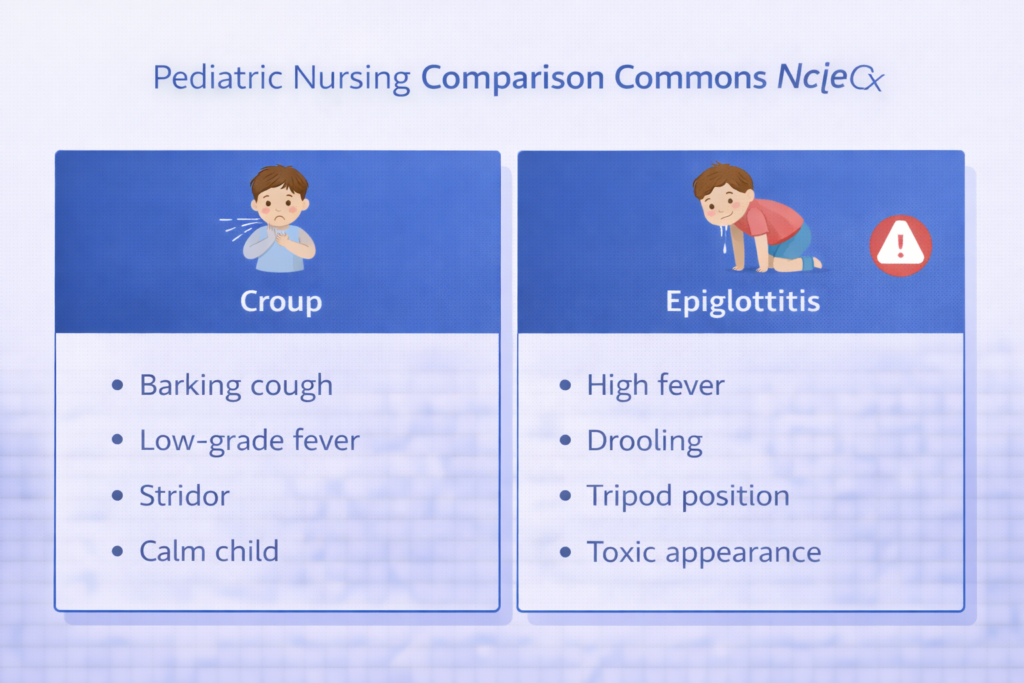
Distinguishing croup from epiglottitis is one of the most frequently tested NCLEX pediatric nursing clinical recognition scenarios. Croup — laryngotracheobronchitis — presents with a barking seal-like cough, inspiratory stridor, and low-grade fever, typically in children 6 months to 3 years of age. The child may be anxious but is not toxic-appearing. Priority nursing care is keeping the child calm — agitation worsens stridor — allowing the caregiver to remain present, and providing humidified cool air. Racemic epinephrine and corticosteroids may be ordered for moderate to severe croup. Epiglottitis is a bacterial emergency presenting with high fever, drooling, a muffled or hot potato voice, the tripod or sniffing position, and a toxic appearance. The child is in severe respiratory distress and airway obstruction can occur suddenly. The critical NCLEX pediatric nursing principle for epiglottitis is to never examine the throat, never place anything in the mouth, and never place the child supine — any of these actions can precipitate complete airway obstruction. Prepare for emergency airway management and notify the physician immediately.
Bronchiolitis and RSV
Bronchiolitis caused by respiratory syncytial virus is the most common lower respiratory infection in infants and a high-yield NCLEX pediatric nursing topic. It presents with rhinorrhea, low-grade fever, tachypnea, wheezing, and retractions in infants typically under 2 years of age. Priority nursing interventions are supportive: positioning the infant with the head elevated, providing humidified oxygen if SpO2 is below 94%, ensuring adequate hydration, and suctioning the nares gently before feeding since nasal congestion significantly impairs feeding in obligate nasal breathers. RSV is transmitted by contact and large droplets — contact precautions and droplet precautions are required. Teaching parents signs of respiratory distress — increased retractions, nasal flaring, cyanosis, poor feeding — is a high-yield NCLEX pediatric nursing discharge teaching topic.
Pediatric Respiratory Distress Recognition
Recognizing respiratory distress in children is a foundational NCLEX pediatric nursing skill that applies across all respiratory conditions. The most reliable early signs of respiratory distress in children are tachypnea — a respiratory rate above the normal range for age — nasal flaring, retractions (suprasternal, intercostal, subcostal, and substernal), and grunting in infants. Cyanosis is a late sign indicating severe hypoxia. Head bobbing in infants — using the neck muscles to assist breathing — is an ominous sign of severe respiratory distress. The key NCLEX pediatric nursing principle is to act on early signs of distress — tachypnea and mild retractions — rather than waiting for late signs like cyanosis, which indicate near-respiratory failure.
Cardiovascular Defects in NCLEX Pediatric Nursing
Congenital heart defects are a consistently tested area of NCLEX pediatric nursing. The exam tests clinical recognition of the two major categories — acyanotic and cyanotic defects — and the nursing management priorities for each.
Acyanotic Defects
Acyanotic congenital heart defects involve left-to-right shunting of blood — oxygenated blood recirculates through the pulmonary system rather than entering the systemic circulation. The most commonly tested acyanotic defects in NCLEX pediatric nursing are ventricular septal defect, atrial septal defect, and patent ductus arteriosus. Clinical presentation includes a characteristic heart murmur, signs of increased pulmonary blood flow — frequent respiratory infections, tachypnea, and easy fatigability — and in large defects, signs of heart failure including poor feeding, diaphoresis during feeding, and failure to thrive. The nursing priority for children with acyanotic defects is monitoring for signs of heart failure, ensuring adequate caloric intake — these infants burn significantly more calories due to increased cardiac work — and teaching parents about activity limitations and infection prevention.
Cyanotic Defects
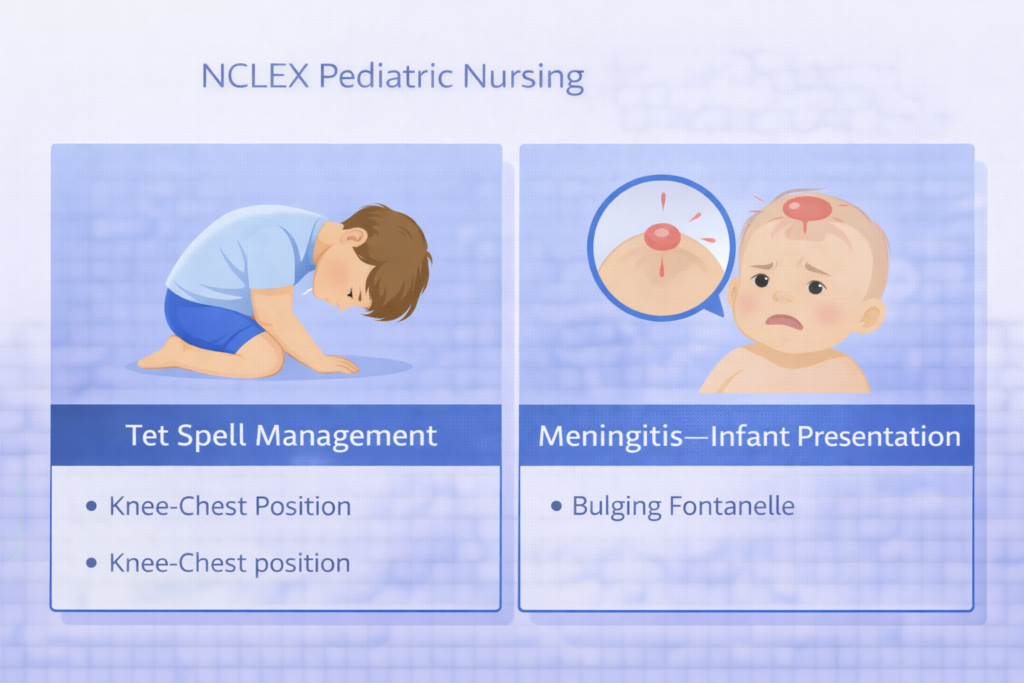
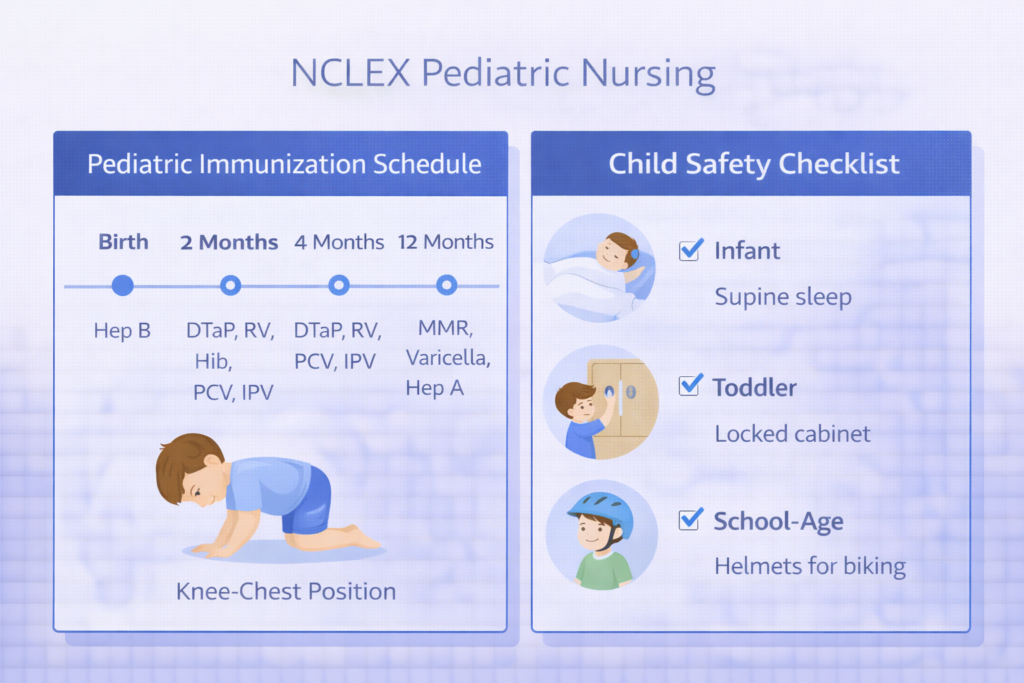
Cyanotic congenital heart defects involve right-to-left shunting, meaning deoxygenated blood enters the systemic circulation and produces cyanosis. The most important NCLEX pediatric nursing cyanotic defect is Tetralogy of Fallot — the most common cyanotic congenital heart defect — which consists of four components: pulmonary stenosis, right ventricular hypertrophy, overriding aorta, and ventricular septal defect. Children with Tetralogy of Fallot experience hypercyanotic episodes — tet spells — characterized by sudden severe cyanosis, hypoxia, and distress triggered by crying, feeding, or defecation. The priority nursing intervention during a tet spell is to place the child in the knee-chest position — also called the squatting position — which increases systemic vascular resistance, reduces right-to-left shunting, and improves pulmonary blood flow. This position is one of the most consistently tested NCLEX pediatric nursing nursing interventions in cardiovascular content.
Neurological and Oncological NCLEX Pediatric Nursing Topics
Febrile Seizures
Febrile seizures are a high-yield NCLEX pediatric nursing topic because they are common, frightening for parents, and require specific nursing management. Febrile seizures occur in children between 6 months and 5 years of age and are triggered by a rapid rise in temperature rather than absolute fever height. The seizure is typically generalized, lasts less than 15 minutes, and resolves spontaneously. Priority nursing interventions during a febrile seizure are identical to those for any seizure: protect the child from injury by clearing the environment, positioning the child on their side, never restraining or placing anything in the mouth, and timing the seizure. After the seizure, assess neurological status and vital signs, administer antipyretics as ordered, and provide clear, reassuring parent teaching: febrile seizures are frightening but rarely dangerous, most children do not develop epilepsy, and parents should call emergency services for any seizure lasting more than 5 minutes.
Meningitis in Children
Bacterial meningitis is a neurological emergency in NCLEX pediatric nursing. Classic findings in older children include high fever, severe headache, nuchal rigidity (neck stiffness), photophobia, and a positive Kernig’s sign — inability to extend the knee when the hip is flexed — and Brudzinski’s sign — involuntary flexion of the knees when the neck is flexed. In infants, presentation is atypical: bulging fontanelle, high-pitched cry, poor feeding, temperature instability, and a rash — petechiae or purpura — indicating meningococcal meningitis. Priority nursing interventions include isolation precautions (droplet for bacterial meningitis), seizure precautions, neurological monitoring, and administering prescribed antibiotics without delay. Patient and family teaching includes the importance of completing the antibiotic course and close contacts receiving prophylactic antibiotics for meningococcal exposure.
Pediatric Cancer — Leukemia
Acute lymphocytic leukemia is the most common childhood cancer and the most heavily tested oncological topic in NCLEX pediatric nursing. The classic presentation is the triad of anemia — fatigue, pallor — thrombocytopenia — petechiae, easy bruising, bleeding — and neutropenia — recurrent infections, fever. The most critical NCLEX pediatric nursing priority for children receiving chemotherapy is neutropenic precautions: the child is at extreme risk for life-threatening infection when the absolute neutrophil count is low. Nursing interventions include reverse isolation, avoiding live plants or fresh flowers in the room, restricting visitors with illness, meticulous hand hygiene, and teaching parents to report any fever in a neutropenic child as a medical emergency regardless of how well the child appears.
Child Safety, Immunizations, and Medication Safety in NCLEX Pediatric Nursing
Developmental Safety Priorities by Age
Child safety is tested in NCLEX pediatric nursing through questions that ask which safety teaching is most appropriate for a child of a specific age. For infants, the priority safety teaching is supine sleep positioning to prevent sudden infant death syndrome, safe sleep environment — firm mattress, no soft bedding — and car seat use from birth. For toddlers, the leading causes of injury are drowning, motor vehicle accidents, falls, and poisoning — teach parents to supervise near water at all times, use rear-facing car seats until the maximum weight limit, install stair gates and window guards, and lock all medications and household chemicals out of reach. For preschoolers, pedestrian safety and stranger safety become priorities. For school-age children, bicycle helmet use, water safety, and firearm safety — if firearms are in the home, store unloaded and locked separately from ammunition — are high-yield NCLEX pediatric nursing teaching topics.
Immunization Schedule and Contraindications
Immunization knowledge is a consistently tested component of NCLEX pediatric nursing. Key vaccines and their timing include: hepatitis B at birth, 1 to 2 months, and 6 to 18 months; DTaP (diphtheria, tetanus, pertussis) at 2, 4, 6 months, 15 to 18 months, and 4 to 6 years; MMR (measles, mumps, rubella) at 12 to 15 months and 4 to 6 years; varicella at 12 to 15 months and 4 to 6 years; and influenza annually after 6 months. The most important NCLEX pediatric nursing contraindication to know is that live attenuated vaccines — MMR, varicella, rotavirus, LAIV flu — are contraindicated in immunocompromised children, including those receiving chemotherapy. Mild illness without fever is not a contraindication to vaccination; this is a commonly tested misconception.
Weight-Based Medication Safety
Medication safety is a critical NCLEX pediatric nursing topic because all pediatric medication doses are calculated on a milligrams-per-kilogram basis, making errors in weight measurement or calculation potentially lethal. Before administering any medication to a pediatric patient, verify the order against the child’s current weight in kilograms, calculate the safe dose range using the prescribed mg/kg dose, confirm the ordered dose falls within that range, and use a second nurse verification for high-alert medications. Teaching parents about home medication safety — using a calibrated oral syringe rather than a household teaspoon, never exceeding recommended doses of acetaminophen, and keeping all medications in child-resistant containers out of reach — is a high-frequency NCLEX pediatric nursing patient teaching scenario.
High-Yield Clinical Reasoning Principles for NCLEX Pediatric Nursing
Beyond individual conditions, NCLEX pediatric nursing tests a set of cross-cutting clinical reasoning principles that apply across every pediatric scenario. Mastering these principles elevates your performance on the full range of pediatric questions the exam presents.
- Always account for developmental stage in your nursing approach: Every NCLEX pediatric nursing question that involves communication, teaching, procedure preparation, or psychosocial support is answered by first identifying the child’s developmental stage and applying the appropriate approach for that stage. Offering a toddler a limited choice, using a doll to demonstrate a procedure for a preschooler, and explaining cause and effect to a school-age child are all developmentally grounded nursing interventions that the NCLEX consistently rewards as correct.
- Normal vital signs vary significantly by age: A respiratory rate of 16 is normal for an adult but indicates serious bradypnea in a neonate whose normal rate is 30 to 60. A heart rate of 100 is mildly elevated in an adult but is normal in a toddler. NCLEX pediatric nursing questions frequently use vital signs as clinical clues — and interpreting them correctly requires knowing the age-appropriate normal ranges, not the adult ranges. Know that respiratory rate, heart rate, and blood pressure all shift significantly across pediatric age groups.
- Children compensate for physiological compromise longer but decompensate faster: Children have strong physiological compensatory mechanisms that allow them to maintain relatively normal vital signs longer than adults during early shock or respiratory compromise. However, once compensation fails, deterioration is rapid. NCLEX pediatric nursing clinical judgment questions test whether you recognize the early, subtle signs of compensation — tachycardia, increased work of breathing, pallor — rather than waiting for the late, obvious signs of decompensation — cyanosis, bradycardia, altered consciousness.
- Pain assessment tools must be age-appropriate: Pain assessment is a critical NCLEX pediatric nursing safety priority. Use the FLACC scale (Face, Legs, Activity, Cry, Consolability) for infants and non-verbal children. Use the Wong-Baker FACES scale for children aged 3 to 7. Use the numeric 0 to 10 scale for children 8 and older who can reliably self-report. Selecting an age-inappropriate pain assessment tool is a nursing error the NCLEX specifically tests, and knowing which tool applies to which age group is a direct knowledge question that appears frequently.

Conclusion
NCLEX pediatric nursing rewards candidates who understand that children are not small adults and who apply that understanding to every clinical scenario the exam presents. Growth and development milestones, Erikson’s psychosocial stages, family-centered care, respiratory distress recognition, congenital heart defects, neurological emergencies, child safety teaching, immunization contraindications, and age-appropriate pain assessment are the must-know topics that appear most consistently in pediatric NCLEX questions.
Approach every NCLEX pediatric nursing question by identifying the child’s developmental stage first, then applying your clinical reasoning frameworks within that developmental context. Practice with targeted pediatric questions daily, review all rationales thoroughly, and track your performance in this content area separately so that any persistent gaps receive the dedicated attention they require. With a developmental, reasoning-focused approach, NCLEX pediatric nursing becomes one of the most clinically coherent and rewarding content areas in your entire exam preparation.
What pediatric topics are on the NCLEX?
The most heavily tested NCLEX pediatric nursing topics are growth and developmental milestones, Erikson’s psychosocial stages and their nursing implications, family-centered care, respiratory conditions including croup versus epiglottitis and bronchiolitis, congenital heart defects including Tetralogy of Fallot tet spell management, febrile seizures, bacterial meningitis in children and infants, acute lymphocytic leukemia and neutropenic precautions, age-specific child safety teaching, the pediatric immunization schedule and contraindications, weight-based medication safety, and age-appropriate pain assessment tools.
How is NCLEX pediatric nursing different from adult nursing?
NCLEX pediatric nursing differs from adult nursing in several fundamental ways: all medication doses are weight-based rather than standardized; normal vital sign ranges differ significantly across pediatric age groups and must not be evaluated against adult norms; nursing communication and procedure preparation must be developmentally appropriate for the child’s stage; family involvement — particularly parent participation in care — is a standard component of every pediatric nursing plan; and children compensate for physiological compromise longer but decompensate more rapidly than adults, requiring earlier recognition of subtle warning signs.
What is the priority nursing action during a tet spell?
The priority nursing intervention during a tet spell in a child with Tetralogy of Fallot is to place the child in the knee-chest position. This position increases systemic vascular resistance, reduces right-to-left shunting across the ventricular septal defect, and improves pulmonary blood flow, relieving the hypercyanotic episode. Keeping the child calm — agitation worsens the spell — and administering supplemental oxygen are concurrent nursing actions. This is one of the most consistently tested NCLEX pediatric nursing interventions in cardiovascular content.
Which pain scale should I use for a 5-year-old on the NCLEX?
For a 5-year-old, use the Wong-Baker FACES pain rating scale, which is appropriate for children aged 3 to 7 who can point to a face that represents how they feel but may not reliably use a numeric scale. For infants and non-verbal children, use the FLACC scale. For children aged 8 and older who can reliably self-report, the numeric 0 to 10 scale is appropriate. Selecting the correct age-appropriate pain assessment tool is a direct NCLEX pediatric nursing knowledge question that appears frequently on the exam.
What are the most important immunization contraindications for the NCLEX?
The most important immunization contraindication for NCLEX pediatric nursing is that live attenuated vaccines — including MMR, varicella, rotavirus, and the live attenuated influenza vaccine — are contraindicated in immunocompromised children, including those receiving chemotherapy or high-dose corticosteroids. A commonly tested misconception is that mild illness without fever is a contraindication — it is not, and vaccination should proceed as scheduled. Severe allergic reaction to a previous vaccine dose or to a vaccine component is also a contraindication that the NCLEX pediatric nursing exam tests.
Leave a Reply