NCLEX med-surg content forms the backbone of the licensing exam. Medical-surgical nursing is the broadest clinical specialty — it encompasses nearly every body system, every major disease process, and the majority of the physiological integrity content that makes up the largest weighted category on the NCLEX. Students who build a strong NCLEX med-surg foundation are better prepared across the entire exam, not just in the sections explicitly labeled as medical-surgical.
The challenge with NCLEX med-surg preparation is the sheer breadth of the content. From heart failure and stroke to postoperative care and wound management, the range of conditions a medical-surgical nurse manages — and that the NCLEX tests — is enormous. Without a strategic approach to prioritization, students can spend weeks reviewing med-surg content and still feel underprepared because they spread their time too broadly across conditions of very different exam weights.
This guide covers the must-know NCLEX med-surg concepts for 2026 — the highest-yield conditions, the priority nursing assessments, the clinical judgment principles, and the postoperative care standards that appear most consistently on the exam. Each concept is presented through the lens of clinical reasoning rather than fact recall, because NCLEX med-surg questions test your ability to apply knowledge to patient scenarios, not retrieve it in isolation.
Why NCLEX Med-Surg Is the Foundation of the Entire Exam
NCLEX med-surg content dominates the physiological integrity category, which accounts for approximately 38 to 62 percent of the NCLEX-RN. Within physiological integrity, the four subcategories — basic care and comfort, pharmacological and parenteral therapies, reduction of risk potential, and physiological adaptation — are all heavily populated with medical-surgical nursing content. Cardiovascular disorders, respiratory conditions, neurological emergencies, renal failure, endocrine crises, postoperative complications, and fluid and electrolyte imbalances are all NCLEX med-surg topics that appear across multiple subcategories and multiple question types.
Understanding NCLEX med-surg content deeply also strengthens your performance on questions that are not explicitly categorized as med-surg. Prioritization questions, delegation questions, and safe care environment questions all draw heavily on med-surg clinical knowledge — you cannot correctly prioritize which patient to see first without understanding the clinical significance of their med-surg presentations, and you cannot delegate safely without knowing which conditions require licensed nursing judgment and which do not.
For these reasons, NCLEX med-surg preparation is not just preparation for one content area. It is the preparation that elevates your performance across the entire exam.
How to Approach NCLEX Med-Surg Content Strategically
The most effective approach to NCLEX med-surg preparation is to organize your study around body systems and to study each condition through a consistent clinical reasoning framework: what is the pathophysiology, what are the priority nursing assessments, what are the expected versus unexpected findings, what are the priority interventions, and what complications require immediate action? This framework mirrors the way NCLEX med-surg questions are built and ensures that your knowledge is organized in the format the exam will test it.
Cardiovascular NCLEX Med-Surg Concepts
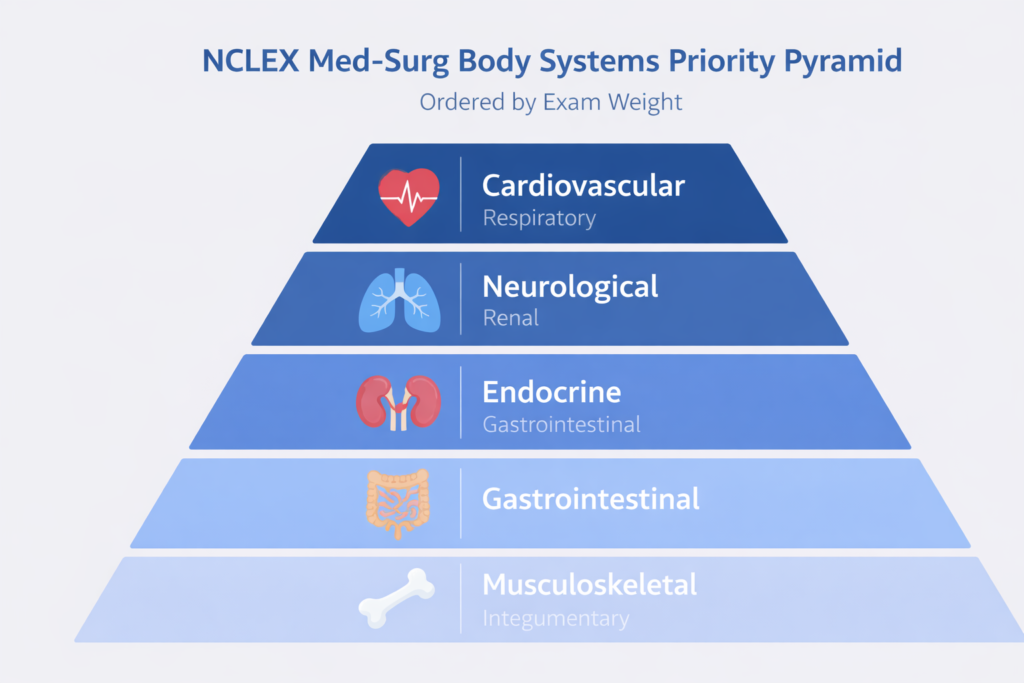
Cardiovascular nursing is the highest-yield NCLEX med-surg content area and deserves the greatest proportion of your study time within physiological integrity. The conditions tested most consistently are heart failure, acute coronary syndromes, cardiac dysrhythmias, and hypertensive emergencies.
Heart Failure
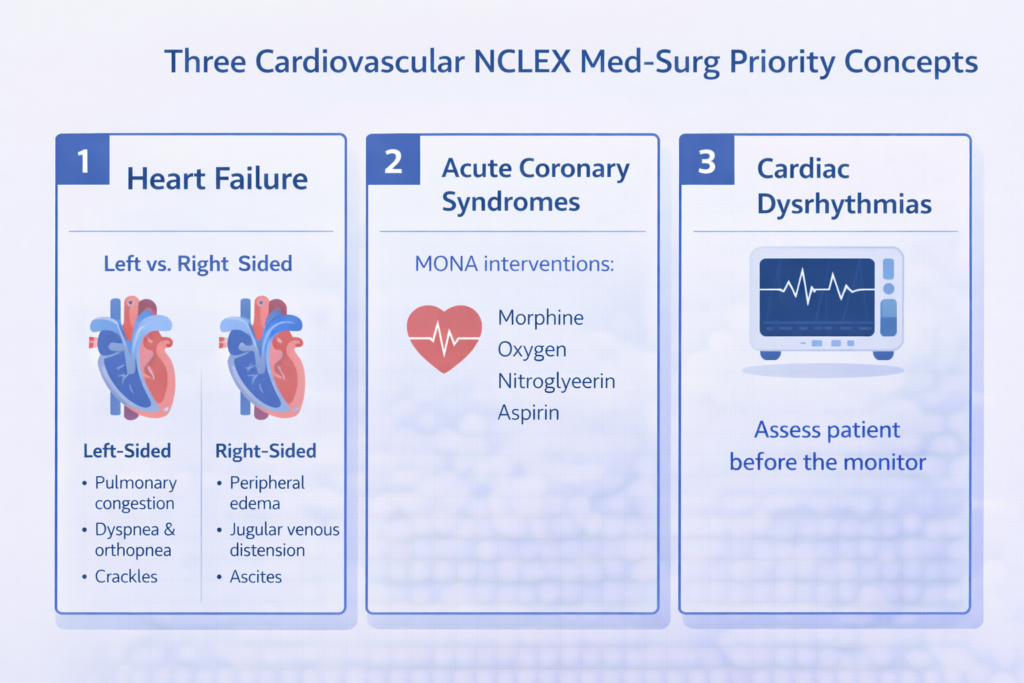
Heart failure is one of the most frequently tested NCLEX med-surg conditions. Know the distinction between left-sided and right-sided failure and the clinical presentation of each. Left-sided failure produces pulmonary congestion — crackles, dyspnea, orthopnea, paroxysmal nocturnal dyspnea, and decreased oxygen saturation. Right-sided failure produces systemic venous congestion — peripheral edema, jugular venous distension, hepatomegaly, and ascites. Priority nursing assessments include daily weight at the same time each day — a weight gain of two or more pounds in 24 hours or five pounds in one week indicates fluid retention requiring provider notification. Nursing interventions include positioning the client upright, restricting sodium and fluid intake, administering prescribed diuretics, and monitoring potassium levels closely when loop diuretics are used.
Acute Coronary Syndromes
Acute coronary syndromes — unstable angina and myocardial infarction — are among the highest-stakes NCLEX med-surg scenarios because the time-sensitivity of interventions directly affects patient outcomes. The priority assessment is the quality and radiation of chest pain — classic MI pain is described as crushing, pressure-like, or squeezing, radiating to the left arm, jaw, or back. The priority intervention mnemonic is MONA: Morphine for pain, Oxygen if saturation is below 94%, Nitroglycerin for vasodilation, and Aspirin to inhibit platelet aggregation. For NCLEX med-surg purposes, know that women, elderly patients, and diabetic patients frequently present with atypical MI symptoms — nausea, fatigue, shortness of breath, or jaw pain without classic chest pain — and that these atypical presentations are a commonly tested clinical recognition scenario.
Cardiac Dysrhythmias
ECG interpretation is a high-yield visual component of NCLEX med-surg cardiovascular content. Know the clinical significance and nursing management of the most commonly tested rhythms: atrial fibrillation — irregular rhythm, absent P waves, risk of embolic stroke requiring anticoagulation — ventricular fibrillation — a lethal rhythm requiring immediate defibrillation — ventricular tachycardia — treat with amiodarone if the patient has a pulse, defibrillate if pulseless — complete heart block — requires pacemaker — and sinus bradycardia — treat with atropine if symptomatic. For all dysrhythmias, the NCLEX med-surg priority is always to assess the patient before treating the monitor: does the patient have a pulse, is the patient symptomatic, and is the patient hemodynamically stable?
Respiratory and Neurological NCLEX Med-Surg Concepts
Respiratory Failure and Oxygenation
Respiratory nursing is the second highest-yield NCLEX med-surg category. Priority conditions include pneumonia, COPD exacerbation, pulmonary embolism, acute respiratory distress syndrome, and pneumothorax. For pneumonia, the priority nursing interventions are positioning the client upright to facilitate breathing, encouraging coughing and deep breathing, administering prescribed antibiotics and antipyretics, and ensuring adequate hydration. For COPD, know the oxygen delivery principle — maintain SpO2 at 88 to 92% in severe COPD to avoid suppressing hypoxic drive. For pulmonary embolism, recognize the classic triad of sudden-onset dyspnea, pleuritic chest pain, and hemoptysis, and know that anticoagulation is the priority intervention. Pneumothorax presents with sudden unilateral chest pain, absent breath sounds on the affected side, and tracheal deviation toward the unaffected side in tension pneumothorax — a medical emergency requiring immediate needle decompression.
Neurological Emergencies
Neurological NCLEX med-surg content centers on stroke, increased intracranial pressure, seizure disorders, and spinal cord injury. For stroke, know the FAST assessment — Face drooping, Arm weakness, Speech difficulty, Time to call 911 — and the critical nursing priority that the time of symptom onset must be established immediately because tPA administration eligibility depends on it. For increased intracranial pressure, know the Cushing’s triad — widening pulse pressure, bradycardia, and irregular respirations — as a late, ominous sign of herniation. Nursing interventions for increased ICP include elevating the head of the bed to 30 degrees, maintaining neutral head and neck alignment, minimizing stimulation, and avoiding Valsalva maneuvers. For seizures, the priority nursing action during a seizure is protecting the patient from injury — side-lying position, padding side rails, never restraining or placing anything in the mouth — and timing the seizure for documentation and provider notification.
Spinal Cord Injury
Spinal cord injury is a high-yield NCLEX med-surg neurological topic because it generates multiple clinical judgment questions about both acute management and long-term complications. Autonomic dysreflexia is the most critical complication to recognize: it occurs in injuries at T6 and above and presents as sudden severe hypertension, bradycardia, pounding headache, diaphoresis above the injury level, and flushing. The priority intervention is to sit the patient upright immediately to lower blood pressure and identify and eliminate the triggering stimulus — most commonly a full bladder or bowel. Autonomic dysreflexia is a hypertensive emergency that can cause stroke or death if not addressed promptly, making it one of the highest-stakes NCLEX med-surg scenarios in neurological nursing.
Renal, Endocrine, and Fluid Balance NCLEX Med-Surg Concepts
Acute Kidney Injury and Chronic Kidney Disease
Renal NCLEX med-surg content focuses on acute kidney injury, chronic kidney disease, and the electrolyte imbalances that accompany renal dysfunction. For AKI, know the three phases — oliguric (urine output below 400mL/day with rising creatinine and BUN), diuretic (dramatically increased urine output with risk of dehydration and electrolyte loss), and recovery. Priority nursing assessments include strict intake and output monitoring, daily weights, and electrolyte levels — particularly potassium, which rises dangerously in oliguric renal failure. For chronic kidney disease, know the dietary restrictions — low protein, low potassium, low phosphorus, low sodium — and the complications: anemia from decreased erythropoietin, hyperphosphatemia causing hypocalcemia, and metabolic acidosis. Dialysis access care — protecting the AV fistula arm from blood pressure cuffs, venipuncture, and compression — is a commonly tested NCLEX med-surg safety topic.
Diabetic Emergencies
Diabetic emergencies are among the most consistently tested NCLEX med-surg endocrine scenarios. Know the clinical distinction between diabetic ketoacidosis and hyperosmolar hyperglycemic state. DKA occurs primarily in type 1 diabetes, presents with blood glucose typically above 250 mg/dL, Kussmaul respirations, fruity breath, nausea, vomiting, and metabolic acidosis. Priority interventions are IV fluid resuscitation and insulin infusion. HHS occurs primarily in type 2 diabetes, presents with extremely elevated blood glucose — often above 600 mg/dL — severe dehydration, and altered consciousness without significant acidosis. Priority intervention is aggressive IV fluid replacement. For hypoglycemia — blood glucose below 70 mg/dL — the priority intervention is the rule of 15: 15 grams of fast-acting carbohydrate, recheck in 15 minutes, repeat if still low. If the patient is unconscious, IV dextrose or glucagon is administered.
Fluid and Electrolyte Imbalances
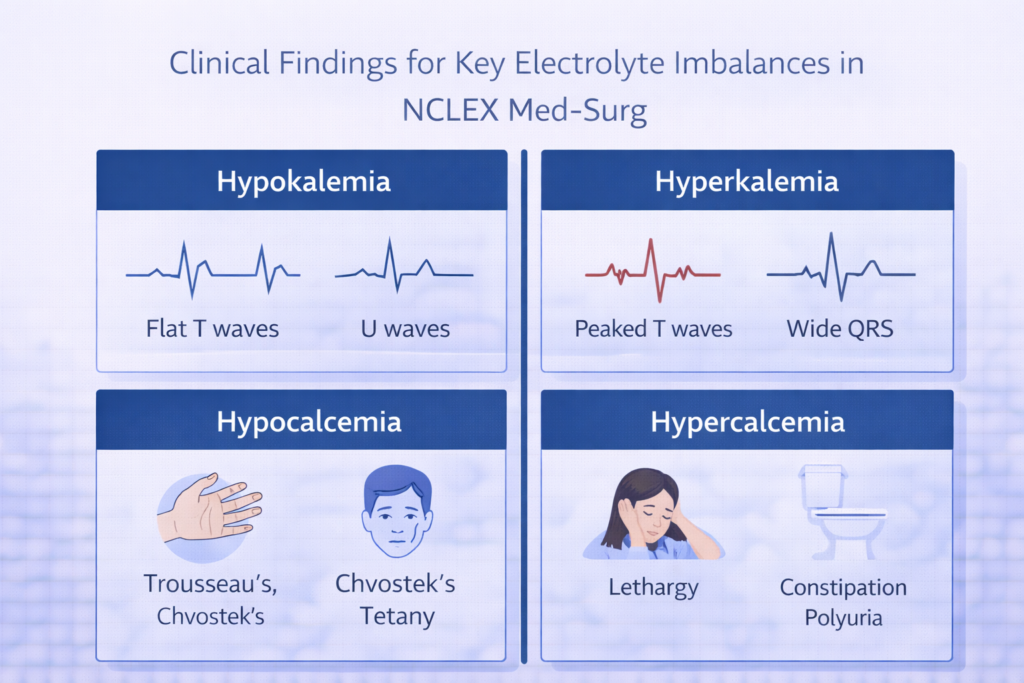
Fluid and electrolyte NCLEX med-surg content is embedded across every body system and represents one of the most consistently tested clinical reasoning areas on the exam. The highest-yield imbalances are hyponatremia and hypernatremia, hypokalemia and hyperkalemia, hypocalcemia and hypercalcemia, and hypomagnesemia. For potassium, know the ECG changes: hypokalemia produces flattened T waves and U waves; hyperkalemia produces tall peaked T waves, widened QRS, and can progress to ventricular fibrillation. For calcium, know that hypocalcemia causes neuromuscular excitability — Trousseau’s sign, Chvostek’s sign, tetany — and that hypercalcemia causes lethargy, constipation, polyuria, and kidney stones. These clinical recognition patterns are the foundation of fluid and electrolyte NCLEX med-surg reasoning.
Postoperative Care in NCLEX Med-Surg
Postoperative nursing care is one of the most consistently tested procedural areas in NCLEX med-surg and one where clinical reasoning questions appear with high frequency. The exam tests your ability to distinguish expected postoperative findings from complications that require immediate intervention.
Immediate Postoperative Assessment Priorities
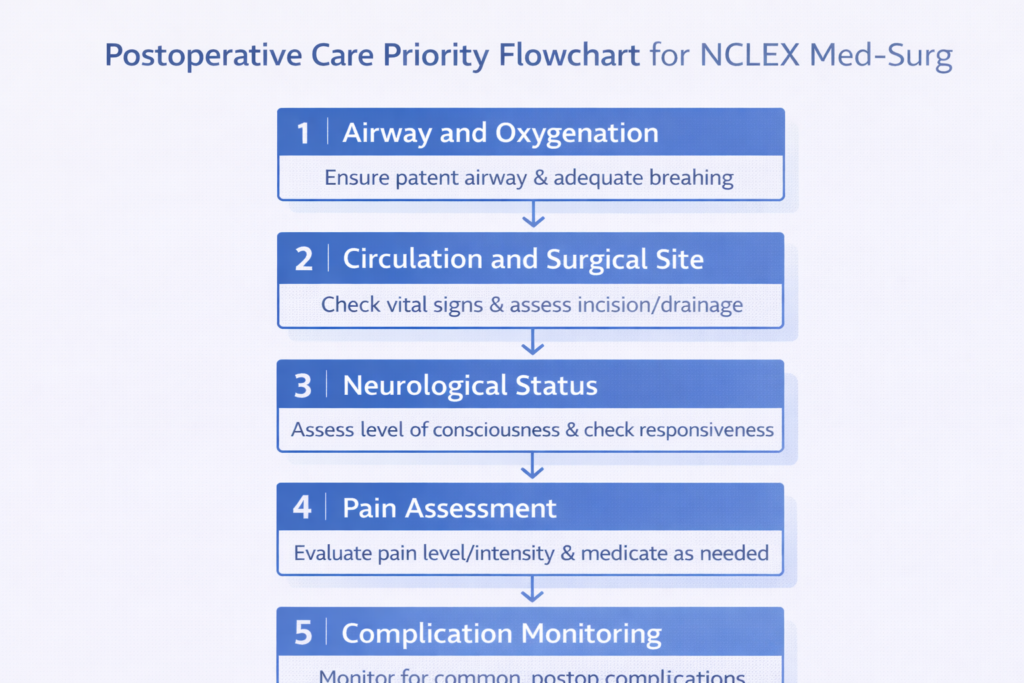
The priority nursing assessment framework for any NCLEX med-surg postoperative scenario follows the ABCs. First, assess airway patency and oxygen saturation — residual anesthesia can suppress respiratory drive, and airway obstruction is the most immediately life-threatening postoperative complication. Second, assess circulation — vital signs, surgical site for bleeding, IV site patency, and urine output. Third, assess neurological status — level of consciousness and return from anesthesia. Fourth, assess pain — using a validated scale and administering prescribed analgesics appropriately. Any postoperative finding that deviates from expected recovery requires immediate assessment and provider notification.
Recognizing Postoperative Complications
NCLEX med-surg postoperative questions frequently ask you to distinguish between expected findings and complications requiring immediate action. Expected findings include mild incisional pain rated three to five out of ten, minimal serosanguineous drainage at the surgical site, low-grade fever up to 38.5°C in the first 24 to 48 hours (atelectasis), and gradual return of bowel sounds. Findings that require immediate intervention include sudden increase in wound drainage — especially bright red arterial bleeding — fever above 38.5°C persisting beyond 48 hours suggesting wound infection, sudden onset of severe pain not relieved by analgesics suggesting hemorrhage or compartment syndrome, absence of urine output for two or more hours suggesting acute urinary retention or AKI, and new-onset confusion suggesting hypoxia, hypoglycemia, or medication reaction.
Deep Vein Thrombosis and Pulmonary Embolism Prevention
DVT and pulmonary embolism prevention is a high-priority NCLEX med-surg postoperative safety topic. The nurse’s role includes early ambulation — the single most effective DVT prevention measure — sequential compression devices applied before and after surgery, anticoagulant prophylaxis as ordered, and leg exercises for immobile patients. Assess for DVT signs — unilateral calf swelling, warmth, and tenderness — and teach patients to report these findings immediately. The complication of a dislodged DVT becoming a pulmonary embolism represents an escalation from a localized med-surg complication to a systemic emergency, and recognizing this escalation trajectory is a clinical judgment skill the NCLEX tests consistently.
High-Yield NCLEX Med-Surg Safety and Clinical Judgment Concepts
Beyond individual conditions, NCLEX med-surg tests a set of overarching safety and clinical judgment principles that apply across every patient scenario. Mastering these cross-cutting concepts elevates your performance on the broad range of med-surg questions that do not fit neatly into a single body system category.
- Recognize the deteriorating patient: One of the highest-yield NCLEX med-surg clinical judgment skills is recognizing when a patient is deteriorating and acting before the situation becomes a crisis. The pattern of early deterioration — subtle changes in level of consciousness, a rising respiratory rate, a heart rate trending upward, a blood pressure trending downward — is more clinically significant than any single abnormal vital sign in isolation. NCLEX med-surg questions test whether you notice these trends and act on them rather than waiting for an acute emergency.
- Understand expected versus unexpected findings: The most reliably tested NCLEX med-surg question pattern is: given this patient and this condition, which finding requires immediate nursing intervention? Answering correctly depends on distinguishing expected findings — consistent with the condition and the stage of treatment — from unexpected findings that represent a new complication or deterioration. Building a mental model of expected findings for every high-yield condition allows you to recognize the unexpected finding instantly when the question presents it.
- Apply wound care and infection control principles: Wound assessment and infection control appear consistently in NCLEX med-surg scenarios. Know the signs of wound infection — erythema, warmth, edema, purulent drainage, fever, increased pain — and the priority nursing actions: culture before antibiotics when possible, wound care per order, and provider notification. Know that methicillin-resistant Staphylococcus aureus wounds require contact precautions, that postoperative wound dehiscence requires covering the wound with a sterile saline-moistened dressing and notifying the surgeon immediately, and that evisceration — protrusion of abdominal organs through the wound — requires covering with a sterile moist dressing and urgent surgical intervention.
- Prioritize pain assessment and management: Pain management is a high-frequency NCLEX med-surg nursing responsibility. The priority assessment before any analgesic administration is a complete pain assessment — quality, location, radiation, severity on a validated scale, and factors that relieve or worsen the pain. For opioid analgesics, assess respiratory rate before and after administration. For non-opioid analgesics, assess liver function indicators for acetaminophen and renal function for NSAIDs. Patient teaching about pain management — what to expect, how to rate pain, when to request analgesics — is a consistently tested NCLEX med-surg topic particularly in postoperative and chronic condition scenarios.

Conclusion
NCLEX med-surg content is the foundation of the licensing exam — and mastering it means more than memorizing disease processes. It means understanding the clinical reasoning patterns that connect pathophysiology to nursing assessment, assessment to priority intervention, and intervention to complication recognition. The highest-yield NCLEX med-surg areas — cardiovascular, respiratory, neurological, renal, endocrine, fluid and electrolytes, postoperative care, and cross-cutting safety principles — each reward candidates who study them through the lens of clinical judgment rather than isolated fact recall.
Build your NCLEX med-surg preparation around body systems, apply a consistent clinical reasoning framework to every condition you review, practice with targeted med-surg questions daily, and prioritize the conditions that carry the highest exam weight and the highest patient safety stakes. With a strategic, reasoning-focused approach, NCLEX med-surg transforms from an overwhelming content mountain into a navigable, confidence-building foundation for your entire exam preparation.
What are the most important med-surg topics for the NCLEX?
The highest-yield NCLEX med-surg topics are cardiovascular conditions including heart failure, acute coronary syndromes, and cardiac dysrhythmias; respiratory conditions including pneumonia, COPD, and pulmonary embolism; neurological emergencies including stroke, increased intracranial pressure, and seizures; renal failure and electrolyte imbalances; diabetic emergencies including DKA and hypoglycemia; and postoperative care including complication recognition and DVT prevention. These areas appear most frequently and carry the highest clinical judgment demand on the exam.
How do you study NCLEX med-surg effectively?
Study NCLEX med-surg by body system using a consistent clinical reasoning framework: pathophysiology, priority nursing assessments, expected versus unexpected findings, priority interventions, and complications requiring immediate action. Integrate pharmacology into each system as you review it. Practice with targeted NCLEX med-surg questions daily and review all rationales in full. Prioritize conditions by exam frequency — cardiovascular and respiratory content deserve the most study time, followed by neurological, renal, and endocrine content.
How much of the NCLEX is med-surg content?
NCLEX med-surg content spans the physiological integrity category, which accounts for approximately 38 to 62 percent of the NCLEX-RN — the largest single category on the exam. Med-surg knowledge also underlies a significant portion of safe and effective care environment questions, particularly delegation and prioritization scenarios. This means that strong NCLEX med-surg preparation benefits your performance across the majority of the exam, not just in explicitly med-surg questions.
What is the priority nursing assessment for any med-surg patient?
The priority nursing assessment framework for any NCLEX med-surg patient scenario follows the ABCs: airway before breathing before circulation. After establishing physiological stability, assess neurological status and level of consciousness, then perform the system-specific assessment relevant to the patient’s condition. For postoperative patients, add surgical site assessment and pain evaluation. Always compare current findings to the patient’s baseline — it is the change from baseline, not the absolute value, that most often signals the need for immediate action.
How do I recognize postoperative complications on the NCLEX?
Recognize NCLEX med-surg postoperative complications by distinguishing them from expected postoperative findings. Unexpected findings requiring immediate intervention include sudden bright red wound drainage suggesting hemorrhage, fever persisting beyond 48 hours suggesting infection, sudden severe unrelieved pain suggesting compartment syndrome or hemorrhage, absent urine output suggesting urinary retention or AKI, new-onset confusion suggesting hypoxia or medication reaction, and unilateral calf swelling suggesting deep vein thrombosis. Expected findings include mild incisional pain, minimal serosanguineous drainage, low-grade fever in the first 24 to 48 hours, and gradual return of bowel sounds.
Leave a Reply