
NCLEX maternal newborn content spans one of the most clinically distinct and high-stakes nursing specialties on the licensing exam. Maternal-newborn nursing covers four interconnected phases — antepartum care during pregnancy, intrapartum management during labor and delivery, postpartum care of the mother after birth, and newborn assessment and care in the immediate neonatal period. Each phase has its own priority nursing assessments, expected versus unexpected findings, and clinical emergencies that the NCLEX tests with regularity.
Many nursing students approach NCLEX maternal newborn content as a separate, self-contained specialty and study it in isolation from their broader clinical reasoning framework. This is a mistake. The clinical judgment principles that guide maternal-newborn nursing — assess before intervene, distinguish expected from unexpected findings, recognize the deteriorating patient, prioritize the greatest physiological threat — are the same principles that govern every other NCLEX content area. The content is distinct, but the reasoning framework is universal.
This guide covers the must-know NCLEX maternal newborn concepts for 2026 — antepartum complications, normal and abnormal labor patterns, fetal monitoring interpretation, postpartum hemorrhage and other complications, and newborn assessment priorities. Each concept is presented through the clinical reasoning lens the NCLEX applies, emphasizing the priority nursing actions and clinical recognition skills that the exam tests most consistently across maternal-newborn scenarios.
Antepartum NCLEX Maternal Newborn Concepts
Antepartum nursing covers the care of the pregnant patient from conception through the onset of labor. NCLEX maternal newborn antepartum questions focus on recognizing normal versus abnormal pregnancy findings, identifying high-risk conditions, and understanding the priority nursing interventions for pregnancy complications.
Warning Signs During Pregnancy
Recognizing warning signs that require immediate notification of the provider is one of the highest-yield NCLEX maternal newborn antepartum skills. The acronym COAST captures the most critical warning signs: Contractions before 37 weeks (preterm labor), fluid Or bleeding from the vagina (ruptured membranes or placenta previa), Abdominal or uterine pain, Severe headache or visual changes (preeclampsia), and Temperature elevation or signs of infection. For NCLEX maternal newborn purposes, any of these findings in a pregnant patient requires the nurse to stop the current activity, perform a targeted assessment, and notify the provider — not to continue routine care and document for later review.
Preeclampsia and HELLP Syndrome
Preeclampsia is one of the most heavily tested conditions in NCLEX maternal newborn antepartum content. It is defined by hypertension — blood pressure of 140/90 or higher on two occasions at least four hours apart — after 20 weeks gestation, along with proteinuria or end-organ dysfunction. Severe features include blood pressure of 160/110 or higher, severe headache, visual disturbances, epigastric pain, and signs of pulmonary edema. The priority nursing interventions for severe preeclampsia are a quiet, low-stimulation environment to reduce seizure risk, continuous fetal monitoring, IV magnesium sulfate for seizure prophylaxis, and antihypertensive medications as ordered. Know that magnesium sulfate toxicity presents as loss of deep tendon reflexes, respiratory depression, and cardiac arrest — calcium gluconate is the antidote and must be at the bedside. HELLP syndrome — Hemolysis, Elevated Liver enzymes, Low Platelets — is a severe variant of preeclampsia requiring immediate delivery regardless of gestational age.
Placenta Previa Versus Placental Abruption
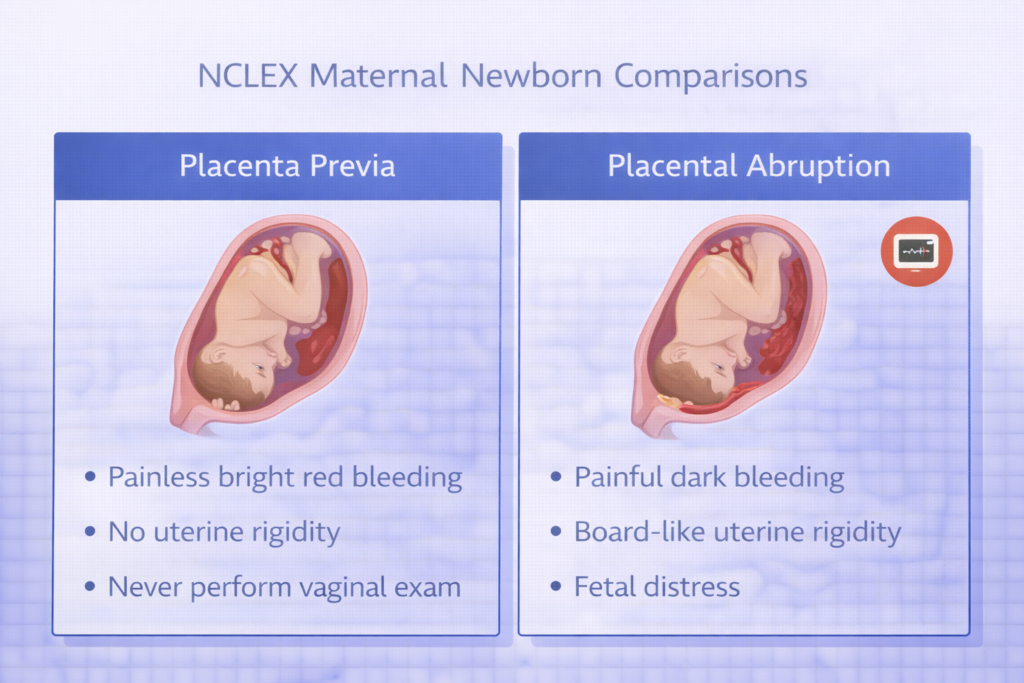
Distinguishing placenta previa from placental abruption is a classic NCLEX maternal newborn clinical recognition scenario. Placenta previa is the abnormal implantation of the placenta over or near the cervical os and presents with painless, bright red vaginal bleeding — typically in the third trimester — without uterine contractions. The absolute priority nursing intervention is to never perform a vaginal examination — doing so can precipitate catastrophic hemorrhage. Placental abruption is the premature separation of a normally implanted placenta and presents with sudden, severe, board-like uterine rigidity and abdominal pain, dark vaginal bleeding (which may be concealed), and fetal distress on the monitor. The distinction — painless bright red bleeding versus painful dark bleeding with a rigid uterus — is one of the most consistently tested NCLEX maternal newborn clinical comparisons on the exam.
Intrapartum NCLEX Maternal Newborn Concepts
Intrapartum nursing covers the care of the patient during labor and delivery — from the onset of regular uterine contractions through the delivery of the placenta. NCLEX maternal newborn intrapartum content focuses heavily on fetal monitoring interpretation, labor progress assessment, and recognition of intrapartum emergencies.
Electronic Fetal Monitoring Interpretation
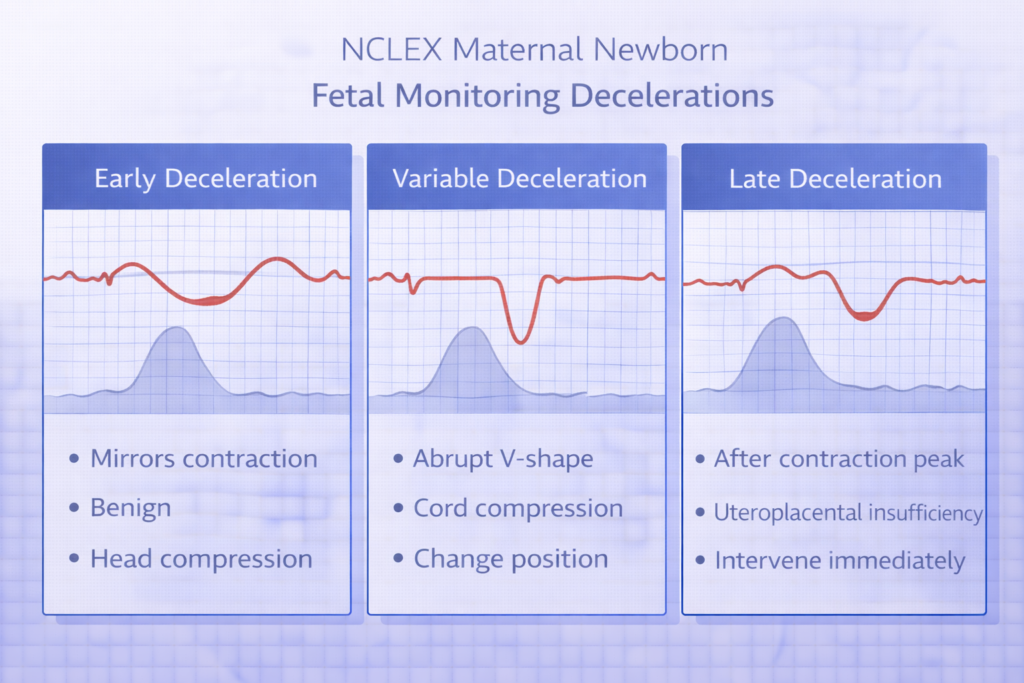
Electronic fetal monitoring interpretation is the highest-yield intrapartum skill in NCLEX maternal newborn content. The baseline fetal heart rate is normal between 110 and 160 beats per minute. Variability — the beat-to-beat fluctuation in the baseline — is the most reassuring sign of fetal wellbeing; moderate variability (6 to 25 bpm fluctuation) indicates an intact, well-oxygenated fetal nervous system. Accelerations — abrupt increases in FHR of 15 bpm or more lasting 15 seconds or more — are reassuring and indicate fetal wellbeing. Decelerations are classified by their timing relative to contractions. Early decelerations — gradual, mirror-image decelerations that begin and end with contractions — are caused by fetal head compression and are benign. Variable decelerations — abrupt, V-shaped, not consistent in timing — are caused by umbilical cord compression and require position changes. Late decelerations — gradual decelerations that begin after the contraction peak and return to baseline after the contraction ends — indicate uteroplacental insufficiency and are the most ominous NCLEX maternal newborn fetal monitoring finding, requiring immediate intervention.
Nursing Response to Late Decelerations
The priority nursing response to late decelerations is one of the most consistently tested intervention sequences in NCLEX maternal newborn intrapartum content. The correct sequence is: reposition the patient to the left lateral position to relieve aortocaval compression and improve placental perfusion, administer supplemental oxygen via non-rebreather mask at 8 to 10L/min, discontinue oxytocin if infusing, increase the rate of the main IV fluid to improve circulating volume, and notify the provider immediately. If late decelerations persist despite these interventions, prepare for emergency delivery. This intervention sequence — position, oxygen, stop oxytocin, IV fluid, notify — is a direct knowledge question that appears across multiple NCLEX maternal newborn question formats.
Intrapartum Emergencies
NCLEX maternal newborn intrapartum emergencies require rapid recognition and an immediate, sequenced nursing response. Umbilical cord prolapse — the cord descending through the cervix ahead of the presenting part — is a obstetric emergency presenting with a sudden severe variable deceleration or prolonged deceleration after rupture of membranes. The priority nursing intervention is to immediately elevate the presenting part manually to relieve cord compression — do not remove the hand until the provider takes over — position the patient in Trendelenburg or knee-chest position, apply a warm saline-moistened dressing to any exposed cord, administer oxygen, and call for emergency cesarean delivery. Shoulder dystocia — impaction of the fetal shoulder behind the maternal pubic symphysis after delivery of the head — is managed with the McRoberts maneuver (hyperflexion of the maternal thighs) and suprapubic pressure (never fundal pressure). These NCLEX maternal newborn emergency scenarios test both recognition and the correct sequenced response.
Postpartum NCLEX Maternal Newborn Concepts
Postpartum nursing covers the care of the mother during the first six weeks after delivery. NCLEX maternal newborn postpartum content focuses on normal postpartum assessment, recognition of hemorrhage and infection, and patient teaching for safe recovery and newborn care at home.
Postpartum Hemorrhage
Postpartum hemorrhage — blood loss greater than 500mL after vaginal delivery or 1000mL after cesarean — is the leading cause of maternal mortality worldwide and the highest-priority emergency in NCLEX maternal newborn postpartum content. The most common cause is uterine atony — failure of the uterus to contract after delivery. Priority nursing assessment is fundal assessment: the fundus should be firm, midline, and at or below the umbilicus. A boggy, soft uterus indicates atony. The immediate nursing intervention for uterine atony is uterine fundal massage, followed by administering ordered uterotonic medications — oxytocin is the first-line agent. Other causes of postpartum hemorrhage follow the 4 Ts: Tone (atony), Trauma (lacerations), Tissue (retained placenta), and Thrombin (coagulation disorders). NCLEX maternal newborn questions test both recognition of hemorrhage signs — excessive lochia, tachycardia, hypotension, pallor — and the priority nursing response.
Postpartum Infection
Postpartum infection — endometritis, wound infection, mastitis, and urinary tract infection — is a consistently tested complication in NCLEX maternal newborn postpartum content. Endometritis presents with fever above 38°C after the first 24 hours, uterine tenderness, foul-smelling lochia, and malaise. Mastitis presents with unilateral breast redness, warmth, swelling, and flu-like symptoms in a breastfeeding mother, typically after the first week. The priority NCLEX maternal newborn teaching point for mastitis is that breastfeeding should continue during mastitis — stopping breastfeeding increases the risk of abscess formation. Encourage frequent feeding or pumping on the affected side, warm compresses, adequate rest, and completion of the prescribed antibiotic course.
BUBBLE-HE Postpartum Assessment
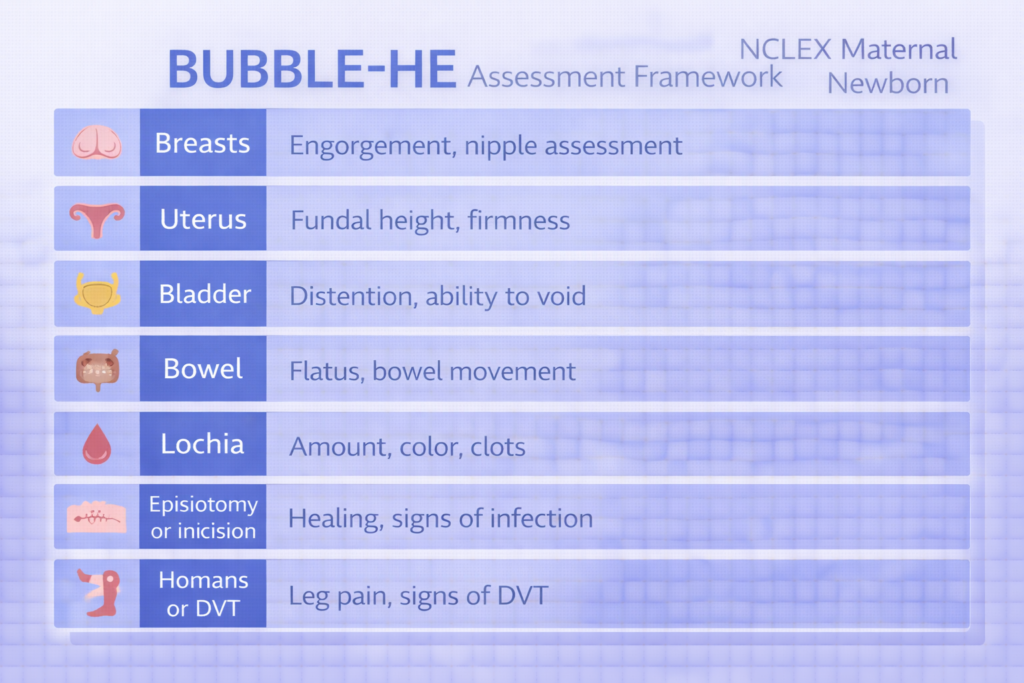
The BUBBLE-HE framework is the standard systematic postpartum assessment framework tested in NCLEX maternal newborn content: Breasts (engorgement, nipple condition, breastfeeding latch), Uterus (fundal height, firmness, position), Bladder (urine output, signs of retention or UTI), Bowel (return of bowel function, constipation), Lochia (amount, color, odor — rubra for days 1 to 3, serosa for days 4 to 10, alba for days 11 to 6 weeks), Episiotomy or cesarean incision (REEDA: redness, edema, ecchymosis, discharge, approximation), Homans’ sign or lower extremity assessment for DVT, and Emotional status (postpartum blues versus postpartum depression versus postpartum psychosis). Distinguishing postpartum blues — transient mood lability resolving within two weeks — from postpartum depression — persistent sadness, inability to care for self or infant — from postpartum psychosis — hallucinations, delusions, and risk of harm to self or infant — is a high-yield NCLEX maternal newborn clinical differentiation question.
Newborn Assessment in NCLEX Maternal Newborn Content
Newborn nursing is a distinct and high-yield component of NCLEX maternal newborn content. The immediate neonatal period — the first hours after birth — requires rapid systematic assessment, recognition of normal adaptive physiology, and identification of findings that indicate compromise.
APGAR Scoring
APGAR scoring is one of the most directly tested knowledge areas in NCLEX maternal newborn newborn content. The APGAR score assesses five parameters at one minute and five minutes after birth: Appearance (skin color), Pulse (heart rate), Grimace (reflex irritability), Activity (muscle tone), and Respiration. Each parameter is scored 0, 1, or 2, for a maximum score of 10. A score of 7 to 10 indicates a vigorous newborn requiring routine care. A score of 4 to 6 indicates moderate depression requiring stimulation and supplemental oxygen. A score of 0 to 3 indicates severe depression requiring immediate resuscitation. The one-minute score guides immediate resuscitation decisions; the five-minute score indicates response to resuscitation and ongoing stability. For NCLEX maternal newborn purposes, the priority nursing action for any APGAR score below 7 is to initiate resuscitative measures — stimulate, warm, dry, and reposition — and prepare for further intervention if the score does not improve.
Normal Newborn Assessment Findings
NCLEX maternal newborn newborn questions frequently present a list of assessment findings and ask which ones require nursing intervention. Knowing which findings are normal and expected prevents false alarms that waste time and generate incorrect answers. Normal newborn findings include: acrocyanosis — bluish discoloration of the hands and feet — which is normal in the first 24 to 48 hours and does not indicate hypoxia; molding of the head from passage through the birth canal; vernix caseosa — a white protective coating on the skin; lanugo — fine downy hair; milia — tiny white papules on the nose and cheeks; Epstein pearls — small white cysts on the hard palate; erythema toxicum — a benign newborn rash; and physiological jaundice, which appears after 24 hours and peaks between days 3 and 5. Jaundice appearing within the first 24 hours is always pathological and requires immediate evaluation — this is a critical NCLEX maternal newborn distinction.
Newborn Thermoregulation and Hypoglycemia
Thermoregulation and hypoglycemia prevention are priority NCLEX maternal newborn newborn nursing responsibilities because newborns are at high risk for both. Newborns lose heat through four mechanisms: evaporation (wet skin), conduction (cold surfaces), convection (air currents), and radiation (proximity to cold objects). Nursing interventions to prevent heat loss include drying the newborn immediately after birth, placing the newborn skin-to-skin with the mother, using warm blankets and a radiant warmer, and delaying the bath until the temperature is stable. Newborn hypoglycemia — blood glucose below 40 to 45 mg/dL — is a risk in infants of diabetic mothers, large for gestational age infants, small for gestational age infants, and preterm infants. Signs include jitteriness, poor feeding, high-pitched cry, lethargy, and seizures. Priority intervention is early, frequent breastfeeding or formula supplementation as ordered.
Key Medications in NCLEX Maternal Newborn Nursing
Medication knowledge is embedded throughout NCLEX maternal newborn content and is tested in both standalone pharmacology questions and clinical scenario questions where the medication is one component of a broader clinical situation.
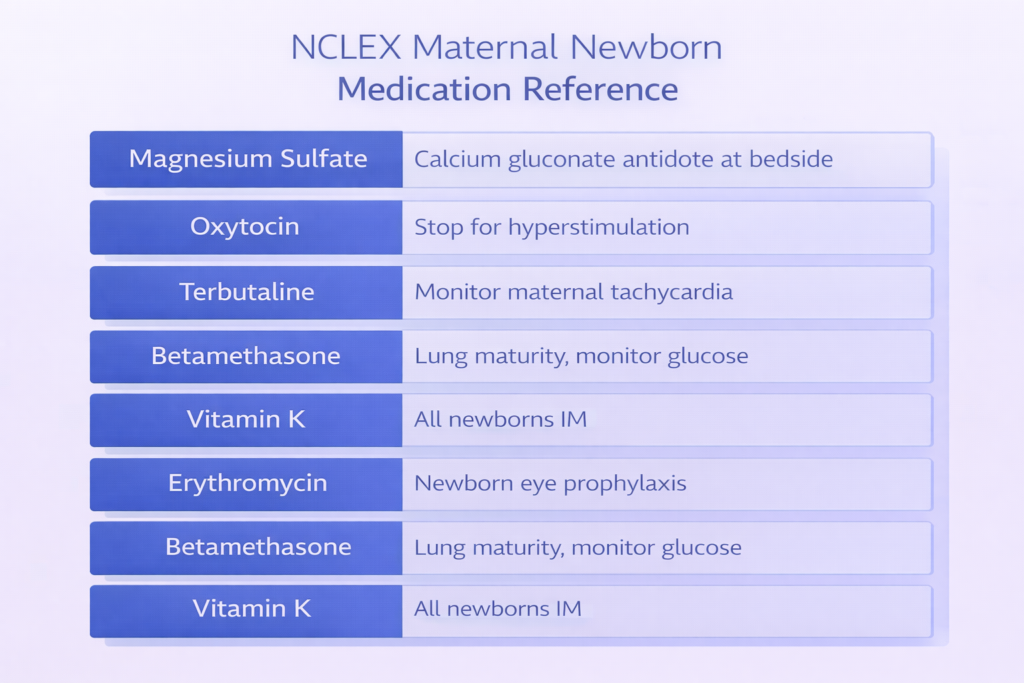
- Magnesium sulfate: Used for seizure prophylaxis in preeclampsia and as a tocolytic for preterm labor. Know the therapeutic range, the signs of toxicity — loss of deep tendon reflexes is the first sign, followed by respiratory depression and cardiac arrest — and that calcium gluconate is the antidote kept at the bedside. Urinary output must be at least 30mL per hour before continuing the infusion, as magnesium is renally cleared.
- Oxytocin (Pitocin): Used to augment or induce labor and to prevent and treat postpartum hemorrhage. During intrapartum use, monitor contraction frequency, duration, and intensity, and assess fetal heart rate continuously. Hyperstimulation — contractions lasting more than 90 seconds or occurring more than five times in ten minutes — requires stopping the oxytocin infusion immediately. Postpartum use is for uterine contraction after delivery.
- Terbutaline: A tocolytic beta-2 agonist used to suppress preterm contractions. Monitor for maternal tachycardia, palpitations, and tremor as expected side effects. Monitor fetal heart rate for tachycardia. Contraindicated if the patient has cardiac disease or uncontrolled diabetes.
- Betamethasone: A corticosteroid given to the mother between 24 and 34 weeks gestation when preterm delivery is anticipated, to accelerate fetal lung maturity and reduce the risk of respiratory distress syndrome in the newborn. Monitor maternal blood glucose — corticosteroids cause hyperglycemia, which requires closer monitoring in diabetic patients.
- Vitamin K (phytonadione): Administered to all newborns intramuscularly after birth to prevent hemorrhagic disease of the newborn, since newborns are born with insufficient vitamin K and lack the intestinal bacteria that produce it. This is a standard, universally administered newborn medication that the NCLEX tests in the context of newborn care teaching.
- Erythromycin eye ointment: Administered to all newborns after birth to prevent ophthalmia neonatorum — a serious eye infection caused by gonorrhea or chlamydia acquired during passage through the birth canal. Application is delayed until after the initial bonding period but administered within one to two hours of birth.
High-Yield Clinical Reasoning Principles for NCLEX Maternal Newborn
Beyond individual conditions and medications, NCLEX maternal newborn tests a set of cross-cutting clinical reasoning principles that apply across antepartum, intrapartum, postpartum, and newborn scenarios. Mastering these principles ensures that your clinical reasoning holds up across the full range of maternal-newborn questions the exam presents.
- When in doubt between mother and fetus, address the life-threatening threat first: NCLEX maternal newborn prioritization questions sometimes present a scenario where both the mother and the fetus show concerning signs. In almost all cases, stabilizing the mother is the priority because maternal physiological stability is the prerequisite for fetal wellbeing. Exceptions exist — cord prolapse management, for example, requires simultaneous action for both — but the default priority is the patient most at immediate physiological risk.
- Distinguish expected from unexpected postpartum findings precisely: The most common NCLEX maternal newborn postpartum question pattern presents a set of findings and asks which one requires nursing intervention. Knowing the exact parameters of expected findings — a fundus that is firm, midline, and at the umbilicus on postpartum day one; lochia rubra that is heavy but not saturating a pad in less than one hour; mild afterpains; and temperature up to 38°C in the first 24 hours — allows you to immediately recognize the unexpected finding that anchors the correct answer.
- Never perform a vaginal examination when placenta previa is suspected: This is an absolute NCLEX maternal newborn rule with no exceptions. If a pregnant patient presents with painless bright red vaginal bleeding, the nurse does not perform a vaginal examination regardless of how routine the situation appears. A digital or speculum examination can precipitate life-threatening hemorrhage by disrupting the placenta. Notify the provider, maintain IV access, monitor vital signs and fetal heart rate, and prepare for ultrasound confirmation.
- Recognize the pattern of preeclampsia escalation: NCLEX maternal newborn preeclampsia questions test your ability to recognize when preeclampsia is escalating toward eclampsia or HELLP syndrome. Blood pressure trending upward despite intervention, new-onset severe headache or visual changes, right upper quadrant or epigastric pain, and decreasing urine output are the cardinal escalation signals. Each of these findings requires immediate provider notification and represents a potential pivot from medical management to emergency delivery.

Conclusion
NCLEX maternal newborn content rewards candidates who understand the full arc of perinatal nursing — from recognizing antepartum warning signs and managing intrapartum emergencies to assessing postpartum complications and performing systematic newborn evaluation. The highest-yield concepts — preeclampsia and magnesium toxicity, placenta previa versus abruption, fetal monitoring deceleration interpretation, postpartum hemorrhage management, BUBBLE-HE assessment, APGAR scoring, newborn thermoregulation, and the key maternal-newborn medications — all appear consistently on the exam and all require clinical reasoning rather than simple fact recall.
Approach every NCLEX maternal newborn question by identifying the phase of care, applying the appropriate assessment framework for that phase, distinguishing expected from unexpected findings, and using the clinical judgment principles that govern every high-stakes nursing scenario. Practice with targeted maternal-newborn questions daily, review every rationale thoroughly, and build your confidence systematically across all four phases of perinatal nursing. With a reasoning-focused, phase-organized approach, NCLEX maternal newborn becomes one of the most clinically coherent and manageable content areas in your entire exam preparation.
What maternal newborn topics are on the NCLEX?
The most heavily tested NCLEX maternal newborn topics are antepartum warning signs and complications including preeclampsia, placenta previa, and placental abruption; intrapartum fetal monitoring interpretation including early, variable, and late decelerations; intrapartum emergencies including cord prolapse and shoulder dystocia; postpartum assessment using the BUBBLE-HE framework; postpartum hemorrhage recognition and management; postpartum infection and mood disorders; newborn APGAR scoring; normal versus abnormal newborn findings; thermoregulation and hypoglycemia prevention; and key maternal-newborn medications including magnesium sulfate, oxytocin, and newborn prophylactic treatments.
What is the priority nursing action for late decelerations on the NCLEX?
The priority nursing response to late decelerations on the NCLEX maternal newborn exam is to reposition the patient to the left lateral position to relieve aortocaval compression and improve uteroplacental perfusion, administer supplemental oxygen via non-rebreather mask at 8 to 10L/min, discontinue oxytocin if it is infusing, increase the IV fluid rate to improve circulating volume, and notify the provider immediately. This sequence — position, oxygen, stop oxytocin, IV fluid, notify — should be applied in order and is a direct knowledge question that appears across multiple NCLEX maternal newborn question formats.
How do you distinguish placenta previa from placental abruption on the NCLEX?
Placenta previa presents with painless, bright red vaginal bleeding without uterine contractions or rigidity — the classic NCLEX maternal newborn distinction. The absolute priority nursing intervention is never to perform a vaginal examination. Placental abruption presents with sudden severe abdominal pain, a board-like rigid uterus, dark or concealed vaginal bleeding, and signs of fetal distress. The uterine rigidity and pain are the defining clinical features that distinguish abruption from previa, and this comparison is one of the most consistently tested clinical recognition scenarios in NCLEX maternal newborn content.
What are the signs of magnesium sulfate toxicity on the NCLEX?
Magnesium sulfate toxicity in NCLEX maternal newborn scenarios presents in a progressive sequence: loss of deep tendon reflexes is the earliest sign and the clinical trigger to hold the infusion and notify the provider, followed by respiratory depression with a rate below 12 breaths per minute, and ultimately cardiac arrest in severe toxicity. Calcium gluconate is the antidote and must be kept at the bedside of any patient receiving magnesium sulfate. Urinary output must be monitored continuously because magnesium is renally cleared — output below 30mL per hour requires holding the infusion and notifying the provider immediately.
What is the APGAR score and how is it used on the NCLEX?
The APGAR score assesses five newborn parameters — Appearance, Pulse, Grimace, Activity, and Respiration — at one minute and five minutes after birth, scoring each 0, 1, or 2 for a maximum of 10. For NCLEX maternal newborn purposes: a score of 7 to 10 indicates a vigorous newborn needing only routine care; a score of 4 to 6 indicates moderate depression requiring stimulation and supplemental oxygen; a score of 0 to 3 indicates severe depression requiring immediate resuscitation. The one-minute score guides initial resuscitation decisions and the five-minute score evaluates response to intervention. The priority nursing action for any score below 7 is to initiate resuscitative measures and reassess.
Leave a Reply